ACDF Surgery: When Is It Considered?
Anterior cervical discectomy and fusion (ACDF) surgery is one of the surgical options used in Singap


Cervical artificial disc replacement (ADR) involves replacing a damaged intervertebral disc with a prosthetic device designed to maintain controlled movement within the cervical spine. It is typically considered in patients with disc degeneration or herniation, causing nerve compression and related symptoms such as neck pain, arm pain, numbness, or weakness.
Through a small incision at the front of the neck (an anterior approach), the surgeon accesses the cervical spine, removes the affected disc, and inserts an artificial disc implant into the disc space. The implant is designed to allow a degree of motion while maintaining spinal stability and relieving pressure on the affected nerve structures.
While traditional cervical fusion surgery (anterior cervical discectomy and fusion, ACDF) stabilises the spine by allowing two vertebrae to heal into a single solid segment, cervical artificial disc replacement (ADR) uses a prosthetic implant intended to preserve motion at the treated level.
Patient selection is a key determinant of outcomes following cervical ADR. The procedure is indicated in specific patterns of cervical disc pathology and is not suitable for all patients with degenerative cervical spine disease.
Cervical ADR is most commonly considered in patients with single-level or, in selected cases, two-level cervical disc herniation resulting in radiculopathy (arm pain, numbness, or weakness due to nerve root compression).
It may also be considered in patients with symptomatic cervical degenerative disc disease who have persistent symptoms despite an adequate trial of structured non-operative management, including physiotherapy, pharmacologic treatment, and activity modification.
Patients with preserved cervical alignment, minimal facet joint arthropathy, and adequate bone quality are generally more suitable candidates. Final suitability is determined based on clinical correlation with imaging findings and overall neurological assessment.
Cervical ADR is generally not recommended in the presence of significant segmental instability, advanced facet joint degeneration, or reduced bone mineral density, such as osteoporosis, due to implications for implant fixation and long-term function.
Other contraindications may include multilevel disease beyond two levels, active infection, or certain inflammatory arthropathies such as rheumatoid arthritis involving the cervical spine. Prior surgical intervention at the intended level may also influence suitability depending on anatomical and biomechanical considerations.
Our neurosurgeon will evaluate clinical presentation, neurological findings, and imaging studies—including MRI and dynamic radiographs where appropriate—before determining the most suitable surgical option.
Cervical ADR surgery is performed under general anaesthesia and typically takes approximately 1–2 hours for a single-level procedure. The patient is positioned supine, and a standard anterior cervical approach is used via a small transverse incision at the front of the neck, typically measuring approximately 3–5 cm.
Soft tissues, including the trachea, oesophagus, and vascular structures, are carefully mobilised to access the anterior cervical spine. Intraoperative fluoroscopy (real-time X-ray guidance) is used to confirm the correct spinal level.
A complete discectomy is performed, with removal of the intervertebral disc and decompression of neural elements. Osteophytes (bone spurs) contributing to foraminal or central canal stenosis are also removed as indicated. The implant achieves initial stability through its design and fixation mechanism, with long-term stability supported by biological integration depending on the implant system used.
In appropriately selected patients, single-level cervical ADR may be performed as a day procedure or with a short inpatient stay of up to 23 hours. Overnight admission may be recommended for multilevel procedures or in patients requiring closer post-operative monitoring based on clinical or medical considerations.
One of the key goals of cervical ADR is to maintain movement at the treated spinal level after surgery. By preserving motion rather than permanently fusing two vertebrae, ADR aims to maintain more natural spinal biomechanics in appropriately selected patients.
Unlike fusion surgery, which eliminates movement at the operated level, ADR is designed to maintain controlled motion between the vertebrae.
Clinical studies have demonstrated that many patients retain movement at the treated segment following surgery. Preserving motion may help maintain more natural neck movement during everyday activities such as looking up, down, and turning the head, although the degree of motion preserved varies between individuals.
One proposed advantage of ADR is the potential to reduce stress on neighbouring spinal levels.
Following fusion, the segments above and below the fused level may experience increased mechanical demands because they compensate for the loss of movement at the operated segment. ADR is intended to maintain motion at the treated level and may help preserve a more normal force distribution across the cervical spine.
While some studies suggest lower rates of adjacent segment degeneration and reoperation following ADR compared with fusion, long-term research is ongoing and individual outcomes may vary.
Many patients are able to resume light daily activities within the first few weeks after surgery, depending on the extent of the procedure and their individual recovery.
Patients with office-based or sedentary occupations may return to work earlier than those whose jobs involve heavy physical activity. Return-to-work timing varies and should follow the recommendations of the treating neurosurgeon based on clinical progress and post-operative assessment.
As with any spinal procedure, cervical ADR carries potential risks. These include both general surgical risks associated with the anterior cervical approach and considerations specific to the artificial disc implant.
Because the cervical spine is accessed through the front of the neck, temporary swallowing difficulty (dysphagia) and hoarseness may occur after surgery.
Most cases improve gradually over the weeks to months following the procedure, although persistent symptoms can occasionally occur. Other potential surgical risks include infection, bleeding, nerve injury, spinal cord injury, and complications related to anaesthesia, though these are uncommon.
As with any implanted device, there are risks specific to artificial disc replacement.
These may include:
Current studies have demonstrated favourable clinical outcomes and durability for many modern cervical disc implants over medium- to long-term follow-up. However, ongoing research continues to evaluate implant performance over longer periods, particularly in younger patients who may place greater lifetime demands on the device.
Recovery following cervical ADR occurs gradually over several weeks to months. While many patients experience early improvement in nerve-related symptoms, recovery timelines vary depending on the underlying condition, the number of levels treated, and individual healing factors.
During the initial recovery period, many patients experience some degree of neck discomfort, incision soreness, or temporary swallowing difficulty. These symptoms generally improve over time.
Light walking is encouraged, while heavy lifting, strenuous exercise, and repetitive neck movements are typically restricted. Wound care instructions should be followed carefully, and any concerns should be discussed with our neurosurgeon.
Some patients notice improvement in arm pain, numbness, or tingling relatively soon after surgery, although nerve recovery may continue for several months.
As healing progresses, patients gradually resume normal daily activities under the surgeon’s guidance.
Many individuals are able to return to office-based or sedentary work during this period, depending on their recovery and job requirements. Gentle range-of-motion exercises or physiotherapy may be recommended where appropriate.
Activity levels are increased progressively, while restrictions on heavy lifting and high-impact activities generally remain in place.
Most patients continue to experience functional improvement over the following weeks and months. Return to more physically demanding activities is guided by symptom recovery, clinical assessment, and follow-up imaging where indicated.
Artificial disc implants are designed to achieve stable fixation within the vertebrae while preserving motion at the treated level. Follow-up appointments allow the neurosurgeon to assess healing, monitor implant position, and provide recommendations regarding return to sport, exercise, and occupational activities.
Recovery timelines vary between individuals, and full recovery may take several months depending on the underlying condition and pre-operative symptoms.
The long-term outcome following cervical artificial disc replacement varies between individuals and depends on factors such as the underlying spinal condition, the severity of nerve compression before surgery, overall health, activity level, and adherence to post-operative recommendations.
The goal of surgery is to relieve symptoms caused by nerve compression while preserving movement at the treated spinal level. Regular follow-up allows the neurosurgeon to monitor recovery, assess implant position, and address any ongoing concerns.
As with any spinal procedure, ongoing care may include activity modification, exercise, physiotherapy, and management of other spinal conditions that may develop over time. Our neurosurgeon can discuss the expected outcomes and long-term considerations relevant to your individual situation.
Before cervical artificial disc replacement (ADR), your neurosurgeon will perform a comprehensive assessment to determine whether the procedure is appropriate for your condition and to ensure you are fit for surgery.
Pre-operative preparation may include:
If you take blood-thinning medications, your surgical team will advise whether any adjustments are required before the procedure. These changes should only be made under medical supervision.
Smoking is associated with impaired healing and may increase the risk of surgical complications. Patients are generally encouraged to stop smoking before surgery, where possible.
It may also be helpful to make practical arrangements for the recovery period, including transportation home after surgery and assistance with daily activities if required.
You should consider evaluation by a neurosurgeon or spine specialist if you experience:
A clinical assessment can help determine whether symptoms may be related to nerve or spinal cord compression and whether further investigation is required.
How long does an artificial disc last?
Cervical artificial discs are designed for long-term use, and available clinical data support durability over medium- to long-term follow-up periods. Ongoing studies continue to evaluate performance over longer durations as more patients are followed over time.
As with any implanted device, long-term monitoring with our neurosurgeon is important to assess implant position, function, and surrounding spinal health.
Will I feel the artificial disc in my neck?
Most patients are not aware of the implant during daily activities. The artificial disc is positioned within the disc space and is designed to move in coordination with the natural motion of the neck.
Some patients may notice mild awareness of movement in the early recovery period, which typically settles as healing progresses.
Can I have an MRI after cervical disc replacement?
Most modern cervical artificial discs are MRI-compatible under specific conditions. This is known as “MR Conditional,” meaning scans can usually be performed safely with appropriate imaging settings.
You should always inform the radiology team about your implant before any MRI scan so that the correct safety parameters can be applied.
What happens if the artificial disc needs further treatment in the future?
In some cases, further treatment may be required if there are ongoing symptoms or implant-related issues. Options may include revision of the artificial disc or conversion to a fusion procedure, depending on the individual situation and clinical findings.
Our neurosurgeon will discuss potential future management options with you as part of the overall treatment planning process.
Cervical ADR is one of several surgical options used to treat cervical disc disease and nerve compression, alongside procedures such as fusion surgery.
ADR may be considered in selected patients to relieve symptoms caused by nerve compression and, in appropriate cases, to preserve motion at the treated spinal level. Suitability depends on individual factors, including the specific spinal pathology, number of affected levels, and overall condition of the cervical spine.
If symptoms persist despite appropriate conservative treatment, a consultation with our neurosurgeon can help determine whether cervical ADR or an alternative surgical approach is suitable.
A detailed clinical assessment, supported by imaging and neurological examination, is required to guide treatment decisions.
Consult with Dr Teo for a comprehensive evaluation and a personalised treatment plan.


Dr Teo Kejia is a Senior Consultant Neurosurgeon and Medical Director at Precision Neurosurgery, with more than 15 years of clinical experience.
Dr Teo has extensive knowledge and experience in the field of neurosurgery, with a particular focus on complex brain tumour procedures. He is adept in employing advanced surgical techniques, including brain mapping and awake brain surgery, especially for treating gliomas and glioblastomas. His expertise extends to neuro-oncology, encompassing both brain and spinal tumours, as well as neurovascular and skull base surgery.
Additionally, Dr Teo offers treatment for a range of neurological conditions, such as traumatic head injuries, intracerebral aneurysms, and degenerative spine disorders, which include neck and back pain. He is also proficient in managing ischemic and haemorrhagic strokes, hydrocephalus, trigeminal neuralgia, and hemifacial spasm.
Have a question or need more information? Please fill in the form below, and our team will assist you.

Anterior cervical discectomy and fusion (ACDF) surgery is one of the surgical options used in Singap

Understand the difference between concussion and structural brain injury. Learn how specialists diag

When your back or neck hurts, you may assume it comes from muscles or joints. In many cases, that is

Brain aneurysm symptoms can resemble migraines or stroke. Learn to recognise warning signs, cranial
Our brains are at the core of everything we do—our thoughts, memories, movements, and even our emo

Degenerative spine conditions refer to disorders that occur when there is a gradual deterioration of

Beyond conventional surgical treatments, awake brain surgery presents the intersection of precision,
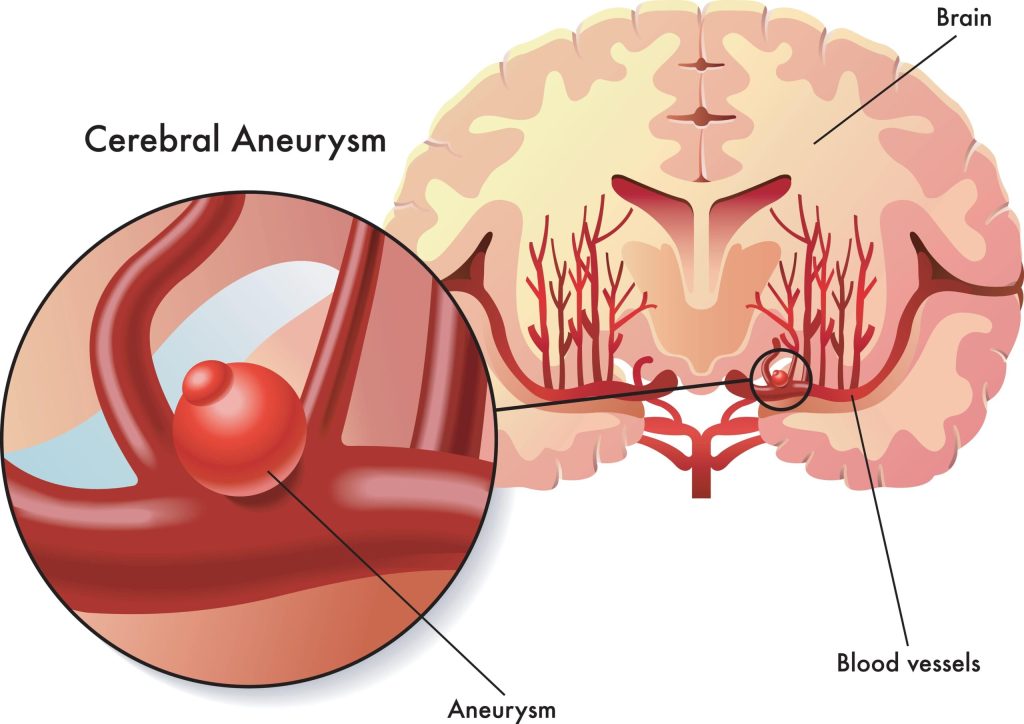
Brain aneurysms can severely impact lifestyle and is best to be treated at the earliest sign. There

Living with a brain tumour can be a daunting journey filled with uncertainty and questions. From und

While occasional headaches are common and often not a cause for concern, frequent headaches accompan