Concussion vs Structural Brain Injury: How Specialists Differentiate Them
Understand the difference between concussion and structural brain injury. Learn how specialists diag


When your back or neck hurts, you may assume it comes from muscles or joints. In many cases, that is true. Muscle strain often causes pain that improves with rest or simple treatment.
However, weakness, numbness, or balance suggest a different cause. These symptoms may point towards nerve involvement. More importantly, they may indicate that your spinal cord is under pressure.
Pain alone does not always mean serious damage. However, changes in strength, coordination, or sensation often suggest a neurological issue rather than a muscular one. When this occurs, proper medical evaluation is important.
Your spinal cord acts as the main communication pathway between your brain and body. It carries signals that control movement, sensation, and balance. Every step you take and every object you hold depends on these signals.
When the spinal cord functions normally, movement and sensation remain coordinated and precise.
A single nerve root supplies a specific area of the body. When a nerve root is compressed, symptoms such as pain, tingling, or numbness typically follow a defined pattern along one limb.
The spinal cord functions differently. It carries signals to and from larger portions of the body. When compression affects the cord itself, symptoms may involve both sides of the body or affect coordination and walking. The impact is broader and potentially more serious.
Spinal cord compression can affect strength, reflexes, and balance simultaneously. You may notice increasing difficulty with tasks that once felt routine.
Because the spinal cord controls multiple functions, even relatively small areas of pressure can lead to noticeable and progressive changes.
Myelopathy refers to dysfunction of the spinal cord. It does not describe a single disease, but rather a pattern of neurological impairment that may result from compression of injury to the cord.
Degenerative changes in the spine can narrow the spinal canal that protects the cord. A disc herniation may press against it. In some cases, tumours or other space-occupying conditions can also contribute to compression.
Myelopathy often develops gradually. Some individuals notice a slow decline in hand coordination or walking stability. Symptoms may not change significantly from day to day, though the pattern can vary depending on the underlying cause and individual factors.
The spinal cord contains upper motor neuron pathways that control movement and coordination. When these pathways are affected, certain characteristic signs deve;op.
Recognising this distinction is important. Symptoms related to muscles or joints often improve with conservative measures. In contrast, ongoing compression of the spinal cord may lead to progressive neurological changes, which is why timely medical evaluation is advisable.
Spinal cord compression may progress if not addressed. Ongoing pressure can affect nerve pathways, and prolonged or severe compression may lead to neurological changes that are more difficult to manage. This is why early evaluation is generally recommended.
The neurosurgeon’s role extends beyond determining whether surgery is required. The assessment includes evaluating neurological findings, interpreting imaging, and identifying the most appropriate management approach for each individual.
Early assessment allows for evaluation before more significant impairment develops. Timely referral may help preserve function and support a broader range of management options. In some cases, delayed evaluation may limit these possibilities.
The neurosurgeon typically evaluates suspected spinal cord involvement through a structured approach:
Symptom history and timeline: The specialist will ask how symptoms began, how they have changed over time, and whether there are associated features such as worsening weakness, numbness, or balance difficulties.
Focused neurological examination: A detailed examination assesses strength, coordination, reflexes, and sensation. Gait and hand function are also observed, as subtle changes may indicate spinal cord involvement.
Targeted imaging review: MRI is the primary imaging modality used to assess the spinal cord, discs, and nerve roots. CT or CT myelography may be considered to evaluate bony structures or when MRI is not suitable. Dynamic X-rays may be used to assess spinal stability.
Correlation of imaging with clinical findings: Imaging results are interpreted alongside clinical findings, as not all abnormalities seen on imaging correspond to symptoms or require intervention. Both are considered together before forming conclusions.
Discussion of findings and next steps: After reviewing symptoms, examination findings, and imaging, the neurosurgeon will explain what the findings may indicate and discuss appropriate next steps. These may include monitoring, further evaluation, or treatment, depending on the individual situation.
Not all cases of spinal cord compression require immediate surgery. When symptoms are mild and stable, careful monitoring and conservative management may be appropriate.
Surgery may be considered when there is progressive weakness, worsening balance, or imaging shows significant compression of the spinal cord. In these situations, the aim of surgery is to relieve pressure on neural structures, reduce the risk of further neurological decline, and help preserve function.
As with all surgical interventions, outcomes vary depending on individual factors, including the severity and duration of compression, overall health, and response to treatment.
Each case is assessed individually, taking into account neurological findings, imaging results, symptom progression, and the patient’s overall condition before any recommendation is made.
Weakness, numbness, and balance problems may reflect more than simple back or neck strain. When these symptoms suggest possible spinal cord involvement, a neurological evaluation can help clarify the underlying cause.Recognising early signs of myelopathy may support more timely management. If you notice progressive neurological changes, seeking assessment from a qualified neurosurgeon in Singapore is advisable.
Consult with Dr Teo for a comprehensive evaluation and a personalised treatment plan.


Dr Teo Kejia is a Senior Consultant Neurosurgeon and Medical Director at Precision Neurosurgery, with more than 15 years of clinical experience.
Dr Teo has extensive knowledge and experience in the field of neurosurgery, with a particular focus on complex brain tumour procedures. He is adept in employing advanced surgical techniques, including brain mapping and awake brain surgery, especially for treating gliomas and glioblastomas. His expertise extends to neuro-oncology, encompassing both brain and spinal tumours, as well as neurovascular and skull base surgery.
Additionally, Dr Teo offers treatment for a range of neurological conditions, such as traumatic head injuries, intracerebral aneurysms, and degenerative spine disorders, which include neck and back pain. He is also proficient in managing ischemic and haemorrhagic strokes, hydrocephalus, trigeminal neuralgia, and hemifacial spasm.
Have a question or need more information? Please fill in the form below, and our team will assist you.

Understand the difference between concussion and structural brain injury. Learn how specialists diag

Brain aneurysm symptoms can resemble migraines or stroke. Learn to recognise warning signs, cranial
Our brains are at the core of everything we do—our thoughts, memories, movements, and even our emo

Degenerative spine conditions refer to disorders that occur when there is a gradual deterioration of

Beyond conventional surgical treatments, awake brain surgery presents the intersection of precision,
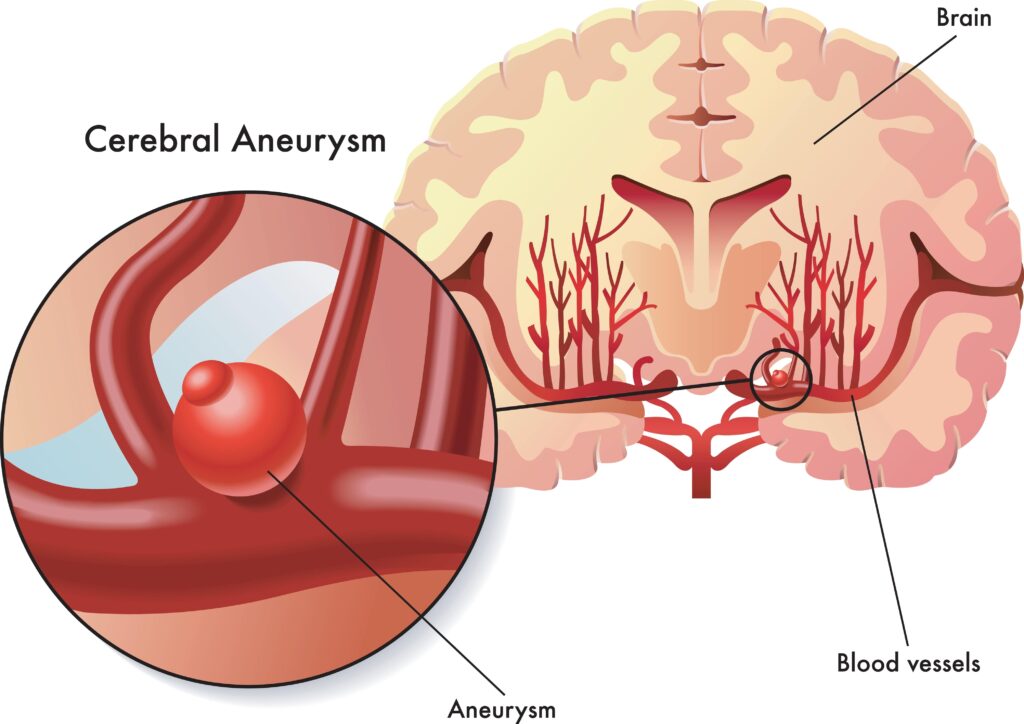
Brain aneurysms can severely impact lifestyle and is best to be treated at the earliest sign. There

Living with a brain tumour can be a daunting journey filled with uncertainty and questions. From und

While occasional headaches are common and often not a cause for concern, frequent headaches accompan

Head injuries, commonly referred to as traumatic brain injuries (TBI), refer to a traumatic experien

Neurological irregularities can impact your life subtly and can be easily shrugged off as tiredness